K-Tape ( Part -2 )

INTRODUCTION
There are 6 current corrective application techniques: mechanical, fascia, space, ligament/tendon, function, and space.
1. MECHANICAL CORRECTION
The Mechanical Correction can be used to either position the tissue in the desired position, provide stimulus in which the body will adjust the position to minimize the created tension or provide a "blocking" action of joint or tissue movement.
there are 3 methods of application:
A. Application of Y technique (Tension on tail )
This technique uses the "recoil" effect of the elastic qualities of the tape to position the tissue in the direction of the base of the Kinesio strip. By using tension in the tails, the practitioner is applying a subtle stimulus.

B. Application of Y technique (With tension on base )
This technique uses the base of the Y cut to apply tension to the skin. The amount of stretch applied to the Kinesio strip and the degree of inward pressure determine the depth and perception of skin movement.

C. Application of I technique ( with tension in tape )
This technique uses the application of tension in the middle of the Kinesio I strip and inward pressure to provide a "blocking" of movement. The amount of tension and inward pressure determine the degree of "blocking".

2. FASCIA CORRECTION
The fascia correction is applied to create and gather fascial tissue to position it in the desired alignment. The tape is applied to hold or assist fascia from unwinding to the unwanted position. This technique is intended to gently break down the limitations of fascia movement via skin movement and elastic qualities of the. Kinesio Tape.
There are 2 methods of application:
A. Use of fascia correction technique to reposition fascia (Tension on the base )
In this technique, the practitioner uses the elastic qualities of the Kinesio Tape to stimulate a manual therapy technique. The elastic qualities of the Kinesio Tape will be applied using an "oscillating" motion in an attempt to reduce tension and adhesions between and within layers of the fascia. This technique may not be as effective as using a manual technique; however, if the practitioner is not skilled in a manual technique this may still allow an option for treatment.

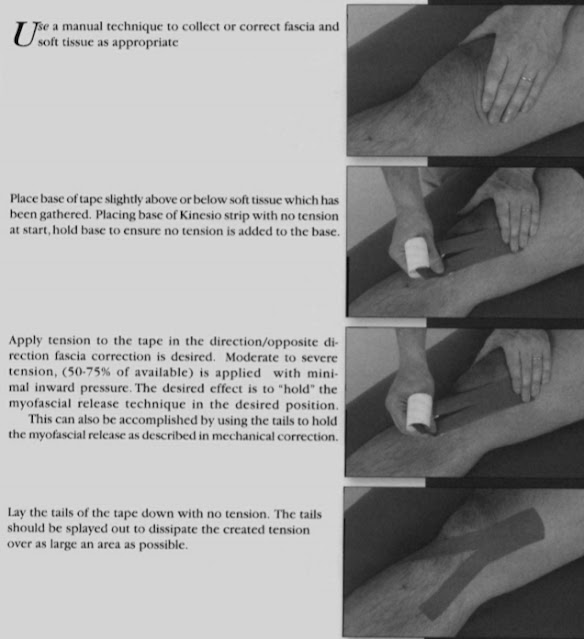
B. Manual fascia winding or myofascial release ( Tension on the base )
Following the application of a manual therapy technique, position the fascia in the desired position before tape application. This technique can be used to either hold fascia in the desired position or limit the movement of the fascia into an unwanted position. Use the Kinesio strip to hold the corrective positioning of the fascia.
3. SPACE CORRECTION
Space correction is applied to create more space directly above an area of pain, inflammation, swelling, or edema. The increased space that is created decreases pressure by lifting the skin directly over the treatment area.
There are 4 methods of application:
A. I- strip
This technique uses the elastic qualities of the Kinesio Tape to lift the skin and create space. This is accomplished by applying tension to the middle 1/3 section of the Kinesio strip and laying down both ends with no tension.

B. Fascia correction
These are fascia correction techniques with the desired therapeutic goal of pain and inflammation reduction.

C. SPACE CORRECTION: Web and Hole technique
The technique uses a hole cut in the center of the Kinesio I strip slightly larger than the area to be treated. The two ends are cut into three tails of approximately 1/3 of the length of the Kinesio strip. The hole is placed directly over the area in which space is to be created.
- Hole technique

- Web technique

4. LIGAMENT / TENDON CORRECTION
The ligament/tendon correction is applied to create increased stimulation over the area of a ligament or tendon resulting in increased stimulation to the mechanoreceptors. This stimulus is believed to be perceived as proprioceptive stimulation that is interpreted by the brain as more similar to normal tissue tension.
There are two methods of correction:
A. Ligament correction
Generally, the base of the corrective strip should be started at the insertion of the ligament. This should ensure the tension being created by the Kinesio strip has a shortening effect on the skin and joints.

B. Tendon correction
proper application of the tendon correction technique will have increased tension, moderate to severe (50-75% of available tension) over the length of the tendon.

5. FUNCTIONAL CORRECTION
functional correction is used when the practitioner desires sensory stimulation to either assist or limit motion. The tape is applied to the skin with no tension during active movement. The tension created by the increased stimulation during active movement is believed to provide stimulation to the mechanoreceptors.


6. LYMPHATIC CORRECTION
lymphatic correction is used to assist in the removal of edema by directing fluid towards a less congested lymphatic pathway and lymph node. This is accomplished by the lifting effect and elasticity of Kinesio Taping. The lifting of superficial skin decreases pressure and opens initial lymphatics.

PRECAUTIONS:
KINESIO TAPING AND DEEP VEIN THROMBOSIS (DVT)
A thrombosis is "the formation, development or existence of a blood clot within the vascular system" (Tabers)
DVT is most often formed in the lower extremities secondary to venous stasis. Postoperative, obese, and sedentary individuals are in the highest danger of developing DVT. They become life-threatening if they dislodge move through the heart-resulting in a pulmonary embolism. They may also be found in the upper extremities as well. Therefore muscle taping is contraindicated if there is any suspicion of DVT.
Superficial Fan Gut taping for edema reduction according to some vascular surgeons is acceptable as it will not affect the tonus of the muscle to dislodge a clot.
KINESIO TAPING FOR SCAR TISSUE
- Do not apply Kinesio Tape directly to a scar until it is well healed.
- Applying tape too early could cause excessive stress to collagen fiber cross-link formation.
- Be extremely cautious with patients with disease processes such as diabetes, venous insufficiency, and peripheral neuropathy.
- Scar correction assists in the softening of scar tissue and reducing adhesions and pitting. It helps to make the scar soft, flat, and pliable.
- Position patient in maximal muscular and fascia/skin elongation of the scarred area. Lay down an I application to adhere to the tape.
- Pitting: Position patient in maximal muscular and fascia/skin elongation of the scarred area. Lay down an I tape with a 75% stretch. Rub the tape after application to adhere to the tape.
- Apply cross strip with 75% tension on tape to lift pitted area.
Comments
Post a Comment